The stock is strained and put into the fridge where the fat rises to the top and solidifies. We take the fat off, put the stock (if it's rich enough, it will have gelled) into ice cube trays and then transfer the frozen cubes into a zip-lock bag where they're handy for making sauces, gravies, stews.
Every now and then though, soup is the only reasonable end product of the stock-making process.

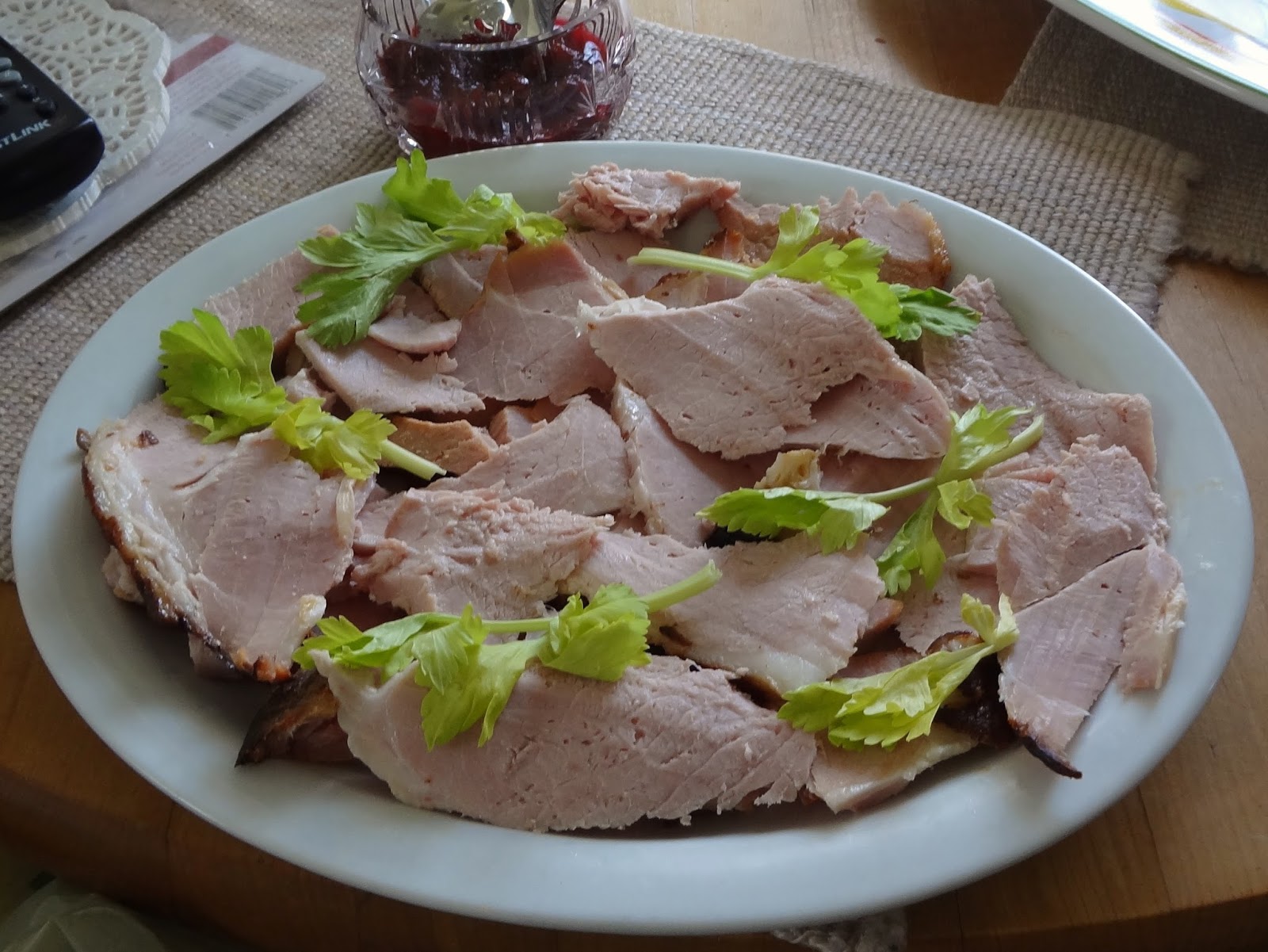
One of our Easter dishes this year was a delectable bone-in, local, organic, smokey ham. This is how it looked the day we served it:

on the counter
on the table
We've had some good meals with the ham since Easter — with pasta, potato scallop, in sandwiches — but it was time for its final act.
Yesterday, I boiled the ham-bone and all the scraps which had been conscientiously saved. The stock went onto the fridge, the fat was taken off, and it was time to make a traditional split pea soup.


I'm one of the people who got one of Jamie Oliver's utility knives in the recent coupon-collecting promotion. It's the one on the upper right (above) and on the left (below). I really like it but the serrated knife has been a favourite for a long time. I also have a large chef-style chopping knife but the truth is, I find it big and it doesn't suit my hand as well as these smaller ones.

I always forget how long it takes to soften those dried peas and if I had it to do again, I'd start them earlier. In fact, if I had it to do again, I'd soak them overnight and then start them earlier.
Everything worked out though. I used the immersion blender and the soup was smooth but still had some texture.


Before serving, I added some chopped ham that had fallen off the bone after the boiling.

It was hearty and filling and we both enjoyed it. I served it with fresh biscuits. This is not a new photo but the biscuits looked much the same today as they did the day this was taken.

I hope you had something satisfying and tasty today. I had fun, not only cooking but taking most of these photos! (Dan took a few also.) I won't do it every day but it's fun now and then.



























